
Annina B. Schmid and Brigitte Tampin
INTRODUCTION
Non-specific low back pain is a common health complaint (mean point prevalence of 18.3%) and is associated with the highest socio-economic burden amongst different chronic pain conditions.1 Spinally referred leg pain is a common variation of low back pain with a prevalence of 1.2% to 43% in the general population.2 Although the prognosis is good in most patients, up to 49% of patients continue to have symptoms for 6 months or longer.3
Low back pain with or without leg pain may be associated with neuropathic pain (pain caused by a lesion or disease of the somatosensory nervous system). A recent meta-analysis suggests that around 36.6% of patients with chronic low back pain may have a neuropathic component.4 The relative contribution of neuropathic components increases with the degree of distal pain radiation into the leg.5 Radiculopathy with associated radicular pain is the commonest neuropathic syndrome in low back pain.
Neuropathic pain is typically associated with more severe pain than purely nociceptive pain.6 In addition, it is accompanied by increased suffering, disability, impaired health-related quality of life and increased health care use. Low back pain with a neuropathic component also poses a significant socioeconomic burden as it increases the already high costs of non-specific low back pain by 45-67%.7 These disproportionally high costs may not only be attributable to the increased pain severity and disability associated with neuropathic pain, but also to our limited understanding of the management of neuropathic pain. This chapter will therefore summarize the current evidence for the pathophysiology, assessment and management of patients with spinally referred back and leg pain with a neural component.
HETEROGENEITY OF SPINALLY REFERRED BACK AND LEG PAIN
The clinical presentation of patients with radiating low back and leg pain is highly heterogeneous. This is reflected in a difference of underlying pain types and related pain mechanisms. On one end of the spectrum are patients with purely nociceptive back/leg pain, for example caused by activation of nociceptors in musculature, joints, ligaments, fascias and tendons. On the other end of the spectrum are patients with frank nerve damage and associated neuropathic pain. Symptoms in neuropathic leg pain may arise from a compromise of the spinal nerve roots, the spinal nerve or the dorsal root ganglia. Patients with lumbar radiculopathy and radicular pain, who in addition to neuropathic symptoms present with impaired impulse conduction within the peripheral afferents, are a classic example of neuropathic leg pain of spinal origin.
It is increasingly recognized that most patients with chronic low back pain with and without leg pain present somewhere on this continuum between “purely nociceptive” and “purely neuropathic.”8 Pain mechanisms often co-exist; for instance, a patient with lumbar radiculopathy may experience leg pain of neuropathic nature (e.g., due to nerve root irritation) as well as focal back pain of nociceptive nature (e.g., due to facet joint degeneration). The determination of the “pain mix” and possible dominance of one pain type is of therapeutic relevance, as neuropathic pain in particular requires specifically targeted management, which is distinct from that of nociceptive pain.
CLASSIFICATION AND CLINICAL PRESENTATION OF SPINALLY REFERRED BACK AND LEG PAIN
A variety of terminologies are used for the description of spinally referred leg pain with a neural component such as sciatica, radicular pain, radiculopathy, neuralgia, neuropathy, neurogenic pain, neuropathic pain, and nerve trunk pain. One difficulty with various terminologies is a lack of consensus in the definition of some of these terminologies. For example, the terms radiculopathy and radicular pain are often used interchangeably in the literature but are in fact different entities.10 We suggest using the following terminology based on pain mechanisms and pathomechanisms: (1) nociceptive somatic back pain, (2) mixed low back pain (nociceptive and neuropathic), (3) somatic referred pain, (4) neural mechanosensitivity, (5) radicular pain, and (6) radiculopathy (see Fig. 10-1). While any of these presentations can occur in isolation, they often co-exist.

Somatic Back Pain/Mixed Back Pain
Nociceptive back pain arises from activation of nerve endings in lumbar structures such as muscles, ligaments, facet joints or fascia. As such, it is characterized by focal hypersensitivity (gain of function; positive sign) in the absence of a neurological deficit (loss of function; negative sign). Pure nociceptive pain remains localized to the area of injury or dysfunction and usually resolves in accordance with expected tissue healing. Patients may use a variety of descriptors for nociceptive pain, including aching, pulling, and dull as well as sharp or throbbing. The behavior of nociceptive pain commonly follows a mechanical pattern, meaning that it can be increased or decreased with specific movements or postures. It can also show ischemic (e.g., increased with prolonged static positions, improvement with movement) or inflammatory components (e.g., night pain, pain after periods of inactivity).
It has been suggested that a subgroup of patients with chronic low back without leg pain may have a mixed nociceptive and neuropathic component. Three mechanisms have been proposed as causes for local neuropathic pain: (i) the lesions of nociceptive sprouts within a degenerated intervertebral disc, (ii) the mechanical compression of the nerve root, or (iii) the inflammatory responses associated with the degenerative intervertebral disc in the absence of any mechanical compression.18 However, objective data for the presence of impaired sensory fiber integrity in the lower back and associated neuropathic pain are still lacking. In the presence of a focal neuropathic component, common neuropathic pain descriptors may be used to describe the pain (see peripheral neuropathic pain below).
Somatic Referred Pain
Nociceptive pain from the lumbar spine may be diffusely referred into locations distant from the injury site. This is labeled somatic referred pain. Proposedly, the mechanism of somatic referral is convergence of nociceptive afferents on second-order neurons in the spinal cord, which also receive input from afferents distant to the injury such as the lower limb.
Classical pain descriptors used for somatic referred pain are dull, aching or pulling pain, which is often diffusely localized.12 It is well established that referred pain from lumbar structures center around the gluteal region, but can lead to extensive pain referral patterns extending all the way into the foot. For instance, zygapophyseal joint referral patterns may extend to the lateral thigh,13 and noxious stimulation of intraspinous ligaments can cause referred pain extending as far as the foot.14 Given the lumbar nociceptive origin, somatically referred pain can often be reproduced or diminished with lumbar movements or postures (mechanical nociceptive) but can also have ischemic or inflammatory components.
Heightened Nerve Mechanosensitivity
A subgroup of patients has vague signs of a nerve disorder without frank nerve damage such as sensory or motor loss, abnormalities on spinal imaging studies or on nerve conduction studies. These patients may present with heightened nerve mechanosensitivity, which is characterized clinically by pain in response to limb movements that elongate the nerve bed and local tenderness on nerve trunk palpation.15 Heightened nerve mechanosensitivity is initiated by activation of nociceptors in the connective tissue sheaths of the peripheral nerve (nervi nervorum) as a consequence of pathology affecting the nerve (inflammation, compression, ischemia). As such, this pain is mostly classified as nociceptive16 and pain descriptors often resemble those used for nociceptive pain. However, if subsequently nerve damage occurs, heightened neural mechanosensitivity can coexist with neuropathic pain.
Radicular Pain
Radicular pain is used to describe spinally referred back and leg pain, which is generated by ectopic firing of neural structures such as the nerve roots and their ganglia or the spinal nerve.10 As such, radicular pain like somatically referred pain is also characterized by gain of function (e.g., increased neural firing); however, the source of pathology is associated with neural structures. Radicular pain usually displays the descriptors of neuropathic pain such as burning, lancinating, electric and shock type pain and is often accompanied by paraesthesia. Radicular pain is said to travel along a narrow band, in the territory supplied by the affected axon. However, clinical studies have shown that most patients report radicular pain in extradermatomal distributions,17 suggesting that the segmental origin of radicular pain cannot be conclusively determined by its distribution.10
Radiculopathy
In contrast to the above conditions, radiculopathy is not defined by the type of pain (gain of function), but by the presence of a neurological deficit (loss of function). In radiculopathy, action potential conduction is blocked or slowed in axons of a spinal nerve or its roots, resulting in a loss of sensory and/or motor function.10,18 Radiculopathy may occur in isolation (without any pain) or in association with radicular pain, somatic referred pain, heightened nerve mechanosensitivity or local spinal pain (Fig. 10-1). For instance, focal nociceptive back pain associated with lumbar radiculopathy might not resolve following surgery that is directed at decompression of neural structures but does not alter nociceptive sources of pain. The frequent combination of nociceptive and neuropathic pain mechanisms in patients with radiculopathy makes their management challenging.
CLINICAL PRESENTATION OF PERIPHERAL NEUROPATHIC PAIN
Peripheral neuropathic pain is generally characterized by pain and sensory abnormalities in the area corresponding to the innervation territory of the damaged nerve structure.19 In addition to pain, the core signs include a sensory deficit, indicating a loss of function due to the reduction of action potential conduction caused by the nerve lesion. In addition to these negative sensory signs, various positive sensory symptoms indicating a gain of function can be present including paraesthesia or dysaesthesia, spontaneous (not stimulus-induced) ongoing pain, spontaneous electric shock like sensations and evoked pain (hyperalgesia, allodynia). Some patients with peripheral nerve injury may however present with positive sensory signs without a demonstrable sensory deficit.20 The quality of neuropathic pain is often described as a shooting or burning quality, with tingling or electrical sensations and numbness. While all the above symptoms, signs and pain descriptors are not universally present, and no single characteristic is pathognomonic for neuropathic pain,21 a combination of sensory descriptors can help to discriminate between nociceptive and neuropathic groups, as demonstrated with the use of various neuropathic pain screening tools22 (see section on neuropathic pain screening tools).
AETIOLOGY AND PHYSIOLOGY FOR RADICULAR PAIN AND RADICULOPATHY
The most common causes for lumbar radiculopathy or radicular pain are disc herniations or spondylotic changes of the vertebral body and facet joints causing foraminal or lateral recess stenosis. However, other aetiologies such as neoplastic, infectious (e.g., herpes zoster, HIV-related polyradiculopathy), inflammatory (e.g., arachnoiditis), and developmental processes (e.g., tethered cord syndrome) may underlie lumbar radiculopathies. Although degenerative changes of the lumbar spine may be very obvious on imaging studies, they do not necessarily correlate with symptom severity. For instance, up to 50-60% of the healthy population have changes to the intervertrebral discs without being symptomatic.23 In contrast, nerve root compromise on MRI only appears in 2-5% of asymptomatic people, suggesting that this may be a more valid imaging finding.24 However, around one third of patients with imaging evidence of nerve root compromise do not have clinical signs of radiculopathy and the extent of radicular leg pain is not proportional to the extent of nerve root compromise.24 Hence, mechanical neural compression per se is not directly related to pain provocation or neurological deficits.
It is however well established that mechanical compression induces significant downstream effects. For instance, experimental compression impairs venular circulation or even halts arterial blood flow in spinal nerve roots.25 The resulting ischemia can slow or block action potential conduction,25 which in turn leads to loss of function (e.g., reduced sensation, muscle weakness, reduced/absent reflexes). Ischemia can however also result in gain of function (e.g., pain, paraesthesia). Intraneural ischemia with associated elevation of lactate levels and a reduction in the activity of Na/K ATPase ion transporters is associated with neuropathic pain behavior in mice.26 The contribution of ischemia to symptoms in radicular pain is supported in patients undergoing discectomy, where an increase in blood flow in the affected nerve root was associated with postoperative pain reduction.27 Prolonged ischemia eventually leads to endoneurial edema and intraneural fibrosis.
Maintained or excessive neural compression or irritation may eventually cause demyelination and axon degeneration. It is well established that direct irritation of the dorsal root ganglion via application of nucleus pulposus material as well as lesions of the peripheral axons (e.g., spinal nerve injury) lead to cell death of sensory neurons. Nerve root compromise also causes upregulation of degeneration markers in dorsal root ganglia neurons, albeit to a lesser extent.28 Axonal degeneration and potential neuronal cell death may explain loss of function as well as delayed postoperative recovery in patients with radiculopathies.
In the past decade, neuroinflammation has gained increasing attention as an important pathomechanism in neuropathic pain. Indeed, it has been shown that even mild nerve compression is sufficient to induce a local inflammatory response with activation of immune cells such as macrophages and T-lymphocytes.29 These immune cells have been closely implicated with neuropathic pain behavior in rodents, mainly via proinflammatory cytokine release and subsequent lowering of neuronal firing thresholds.30 There is a growing body of evidence confirming that neuroinflammation is an important mechanism in radicular pain. For instance, experimental studies suggest that the sheer presence of nucleus pulposus material in close proximity to nerve roots triggers an intraneural inflammatory response locally as well as in associated dorsal root ganglia and the spinal cord with release of inflammatory cytokines.31 The resulting non-compressive nerve root inflammation is associated with increased excitability and mechanical hypersensitivity of dorsal root ganglia neurons and subsequent neuropathic pain behavior in rodents.32 Such neural sensitization may explain the reproduction of radicular pain following intraoperative gentle mechanical manipulation of involved or inflamed lumbar nerve roots, whereas mechanical stimulation of unaffected nerve roots remained painfree.33 In addition to hyperexcitability and neuropathic pain, experimental non-compressive neuroinflammation also causes axonal swelling and demyelination with subsequent nerve conduction slowing,34 which explains the loss of function in radiculopathy. In patients, proving a contribution of an immune-inflammatory response to neuropathic symptoms remains challenging due to limited access to tissues. There is, however, growing evidence from blood and cerebrospinal fluid analysis that inflammation may play a role at least in some patients with lumbar radicular pain. For instance, Pedersen et al.35 found an association of increased serum expression of IL-6 and IL-8 and higher symptom levels in patients with lumbar radicular pain. Interestingly, higher levels of IL-6 have been associated with poorer recovery.36 In another study, serum inflammatory markers were normal in patients with lumbar radicular pain; IL-8 was, however, elevated in the cerebrospinal fluid in a subgroup of patients.37 Recently, researchers have used simultaneous PET and MR imaging to demonstrate increased neuroinflammation in the nerve roots and spinal cord of patients with lumbar radicular pain.38 Sensitization of nerve tissue by inflammatory infiltrates may be responsible for the clinical observation of heightened neural mechanosensitivity. Animal studies have documented that induced inflammation renders intact nerve fibers mechanosensitive to pressure and stretch in the absence of any concurrent signs of axonal damage.39 Neural mechanosensitivity has also been attributed to epineural inflammation with sensitization of nervi nervorum. Electrophysiological studies demonstrated that at least some of the nervi nervorum function as nociceptors.40 Indeed, the nervi nervorum increase their mechanosensitivity if exposed to an inflammatory environment.41 As such, sensitization of the nervi nervorum or axons directly may contribute to heightened nerve mechanosensitivity upon mechanical provocation (e.g., palpation, provocative maneuvers such as straight leg raise) even if nerve conduction (assessed by electrodiagnostic tests and bedside neurological examination) is preserved. Taken together, the pathomechanisms involved in radicular pain and radiculopathy are multifaceted, including mechanical, ischemic and inflammatory components, which can explain the neurophysiological and structural changes resulting in gain and/or loss of function in individual patients. It is well established that nociceptive and neuropathic pain can be associated with nociplastic phenomena, such as central sensitization leading to increased responsiveness of nociceptive neurons in the central nervous system to their normal or subthreshold afferent input.18 Central sensitization is associated with pain that is disproportional and prolonged compared to the noxious stimulus and extends beyond the site of injury (secondary hyperalgesia). Nociplastic mechanisms are commonly present in patients with low back pain but are not the focus of this chapter.
ASSESSMENT OF PATIENTS WITH SPINALLY REFERRED BACK AND LEG PAIN
The differential diagnosis of patients with low back pain and/or spinally referred leg pain is based on findings of a comprehensive clinical examination incorporating the patient’s medical history, an assessment of both musculoskeletal and related neural tissues and a neurological bedside examination of somatosensory and motor function. During the subjective examination, attention is given to pain drawings and the precise pain location and distribution, pain descriptors (nociceptive/neuropathic), the intensity of pain and the pain behavior over 24 hours. The patient’s history provides information on potential mechanisms of injury or causes leading to the pain disorder and possible neurological lesions/disease. Results of medical investigations (e.g., imaging, electrodiagnostic tests) may aid in the diagnostic work-up; however, as mentioned earlier, clinical findings do not always correlate with radiological findings. Nerve conduction studies also have limitations as diagnostic tools for radiculopathies including the fact that they can only assess the function of large, but not small, nerve fibers, which are affected early in patients with entrapment neuropathies.42,43
Peripheral Neurological Examination
Assessment of motor function
The assessment for motor function includes myotomal reflex and strength testing. Commonly examined reflexes of the lower limb include the Achilles tendon reflex (S1), biceps femoris reflex (L5/S1), semimembranosus and semitendinosus reflex (L5), and knee jerk (L3/4). The muscle to be examined is placed in a lengthened position and the contact of the reflex hammer should be at a right angle to the tendon or muscle fibers. Reflexes are graded as increased, reduced or absent. As ankle or patellar reflexes may be reduced in healthy people above 60 years of age,44 reduced reflexes, especially in older patients, should not be interpreted in isolation but within a sound clinical reasoning framework. Table 10-1 documents the myotomes of the lower limbs. Isometric muscle strength testing is performed for the relevant key muscles as a screening test. The muscles to be examined should be tested in their mid-position, with gradually increasing resistance. If myotomal weakness is found, it can be graded using a scale from 0 to 5 according to the Medical Research Council scale for muscle strength.45
| Nerve Root Level | Movement Associated with Myotome |
| L2 | Hip flexion |
| L3 | Knee extension |
| L4 | Ankle dorsiflexion with inversion |
| L5 | Great toe extension |
| S1 | Ankle dorsiflexion with eversion |
| S1 | Ankle plantar flexion |
| S2 | Toe flexion, knee flexion |
Assessment of sensory function
Bedside sensory testing should include the assessment of large (Ab-) and small nerve fiber function (Ad and C-fibers) as both fiber populations may be affected in lumbar radiculopathies46 and associated neuropathic pain. Recommended measures for screening tests are the assessment of light touch sensation with a cotton swab or cotton wool exploring the function of Ab- fibers. Von Frey hairs or the Rydel-Seiffer tuning fork are cost-effective tools to quantify Ab- fiber function so that it can be reassessed at a later time point. A neurotip or toothpick can be used to explore the ability to perceive sharp stimuli mediated by small myelinated Ad-fibers.47 Small fiber function can be assessed in more detail with warm and cold objects such as a tip-therm, warm/cold coins, metal thermoroller or test tubes filled with hot and cold water (Table 10-2). However, thermal testing is more time consuming and, therefore, not often included in standard neurological screening. For a detailed examination of dermatomes of the lower limb, the cotton wool/neurotip is moved circularly around the upper and lower thigh, and upper and lower leg. The dermatomes of the foot are assessed individually on their dorsal and ventral aspects. Any changes in sensation compared to the asymptomatic side are recorded. In case of bilateral symptoms, findings can be compared to a distal or proximal symptom free area or a remote body site such as the abdomen (Table 10-2).
| Type of Stimulus | Axon Type | Tool | Sensory Loss | Sensory Gain | |
|---|---|---|---|---|---|
| Static light touch | Aβ | Q-tip, cotton wool |  |
||
| Vibration | Aβ | Tuning fork |  |
||
| Dynamic mechanical | Aβ | Brush, cotton wool, Q-tip |  |
||
| Pin prick | Aδ and C | Toothpick, neutrotip |  |
||
| Cold/warm detection | Aδ and C | Cold and warm thermorollers/coins test-tubes, thermtip |  |
Somatosensory changes may present as a loss of function (analgesia, hypoesthesia) and/or gain of function (hyperesthesia/allodynia) as well as dysaesthesia. The area of altered sensation can be precisely mapped and recorded on a body chart to observe potential changes over time. To map the borders of an area with loss of function, the test instrument is moved from the region of reduced sensation towards the region of normal sensation. In case of gain of function, testing is performed from the region of normal sensation toward that of increased sensation. Any abnormalities identified in the sensory screening test can be quantified for use as outcome measures.
While dermatomal loss of function is indicative of a nerve root injury/compromise, it does not indicate the presence of neuropathic pain. For the assessment of neuropathic pain, sensory testing has to be performed in the patient’s main pain area,47 which for patients with back and leg pain mostly relates to their leg pain or lower back pain. One has to be mindful with the interpretation of sensory findings, as positive signs, such as hyperalgesia or allodynia, are common in nociceptive pain disorders,48 and subtle negative signs have also been reported in patients with musculoskeletal, non-neuropathic pain.48 However, the border of sensory loss may assist in the interpretation, as in neuropathic pain states the borders correlate with the anatomical distribution of the affected neural structure whereby the borders in nociceptive pain disorders may be diffuse and not reproducible.47
Quantitative sensory testing
Quantitative sensory testing (QST) has gained increasing interest as a method to quantify somatosensory changes both in clinics as well as in research. Compared to bedside assessment, QST allows a more precise and reliable assessment of the magnitude of sensory loss and quantification of thermal and mechanical hyperalgesia/allodynia.49 In contrast to nerve conduction studies which can assess only a loss of function in myelinated nerve fibers, QST can also assess small nerve fiber function as well as both loss and gain of function. Sensory aberrations measured in the skin may be due to a dysfunction anywhere along the sensory pathway between the peripheral sensory receptor apparatus and the brain. Thus, while QST can be used to support a hypothesis as to whether or not a nerve lesion is present, it cannot indicate the location of the lesion.
QST is a psychophysical assessment, in which participant’s responses are influenced by cognitive factors, psychosocial and psychological components. Furthermore, factors such as age, gender, site of stimulation, the environment of a test laboratory and instructions given to the participants have an impact on QST measures. Therefore, standardization of testing protocols is important to facilitate reliability and comparison of QST data between studies. The German Research Network on Neuropathic Pain has developed a highly standardized QST protocol comprising the somatosensory sub-modalities that are mediated by different primary afferents (C-, Ad-, Ab-), and reference data have been obtained for various body regions.49-51
QST is a valuable tool to characterize painful syndromes and to help interpret the pain mechanisms underlying clinical pain presentations. Using QST, subgroups of patients with distinct sensory profiles have been identified in patients with lumbar radicular pain.52 It is postulated that differences in sensory profiles and underlying pain mechanisms may account for differences in responsiveness to pharmaceutical intervention targeting neuropathic pain associated with radiculopathy.52 QST has also been employed in patients with lumbar radiculopathy to assess the recovery of sensory nerve fiber function in the affected dermatomes after lumbar decompression.53,54
ASSESSMENT OF HEIGHTENED NERVE MECHANOSENSITIVITY
Patients with features of heightened nerve mechanosensitivity often present with pain that follows the course of the affected nerve trunk,55 causing a similar distribution as radicular pain. The pain can be provoked or aggravated by spinal and/or limb movements that cause elongation of the affected nerve. Depending on the severity of heightened nerve mechanosensitivity, patients may present with antalgic postures and with painful movement impairment due to the evoked pain response. The latter can be examined with active movements as well as with specific neural provocation tests (NPT); straight leg raise test being the most widely used test in patients with spinally referred leg pain. Nerve trunk palpation may further aid in the assessment of mechanical nerve sensitivity.
The response of a patient to a single NPT is of limited value for the identification of heightened nerve mechanosensitivity. Test responses must be interpreted within the clinical context of a number of other assessment procedures before a classification of heightened nerve mechanosensitivity can be made. The following findings may be part of the clinical algorithm pointing towards heightened nerve mechanosensitivity:15 (1) antalgic posture protecting neural tissue, (2) a correlating active movement dysfunction (e.g., limitation of lumbar flexion), (3) an abnormal response to an NPT, and (4) an abnormal response on nerve trunk palpation.
Antalgic Posture
Figure 10-2 demonstrates a neurally protective posture in a patient with severe left-sided lumbar spine symptoms radiating into the left leg. The patient stands with slight knee flexion and left lumbar side flexion to reduce mechanical provocation (tension) of the sensitized nerve root. This pattern may be indicative of heightened nerve mechanosensitivity.

Another common antalgic pattern is contralateral lumbar side flexion, which opens up the ipsilateral foramen, thus reducing mechanical compression of the affected nerve root.
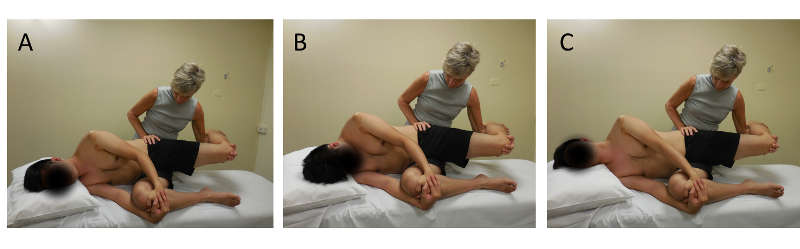
Active Movements
Lumbar flexion, hip flexion, knee extension and foot dorsiflexion cause increased tension on the sciatic nerve, its distal branches and the L4-S2 nerve roots.56 In the presence of heightened mechanosensitivity of these neural structures, lumbar flexion and contralateral side flexion are likely restricted in range due to pain provocation (Fig. 10-3(A)). The movement restriction is greater with the addition of dorsiflexion of the foot as dorsiflexion further increases tension of lumbosacral nerve roots during hip flexion56 (Fig. 10-3(B)).
In case of anterior thigh pain and the suspicion of femoral nerve involvement, the testing maneuver has to be altered according to the anatomical course of the femoral nerve (Fig. 10-3(C)), i.e., hip extension, knee flexion and spinal contralateral side flexion.

Neural Provocation Tests
Neural provocation tests (NPT) use sequences of passive joint movements that cause increased movement, elongation and tension on neural structures. NPTs may provoke a painful response in healthy people, which is a normal physiological response. An abnormal response to an NPT in symptomatic patients is defined as at least partial reproduction of the patient’s symptoms together with positive structural differentiation.57 Structural differentiation uses movements at a site remote to the painful area to further load or unload the nervous system, thus differentiating symptoms of neural origin from local musculoskeletal origin15 (e.g., ankle dorsiflexion added to straight leg raise). In case of pain of neural origin, the pain response is enhanced with increased loading of neural structures and decreased with unloading maneuvers.
Depending on the degree of pain irritability/severity, individual movements are performed to the end of range, or to the onset of pain. If there is constant severe pain, movements may be used to alleviate pain. Upon pain provocation/alleviation, structural differentiation maneuvers are performed. Figures 10-4, 10-5 and 10-6 illustrate the positions for straight leg raise testing (Fig. 10-4), femoral nerve test (Fig. 10-5), and slump test (Fig. 10-6), including structural differentiation maneuvers. Further details on the performance of NPTs, their normal test responses and reliability and validity have been previously documented.58


Palpation of Peripheral Nerves
Palpation of the following peripheral nerves in the lower limbs may be performed: sciatic nerve, common peroneal nerve, peroneal nerve, tibial nerve, sural nerve, femoral nerve and lateral femoral cutaneous nerve. Nerve palpation may be painful even in healthy subjects. Therefore, an abnormal response entails differences in pain responses between sides, i.e., if nerve palpation provokes a pain response on the symptomatic, but not on the asymptomatic side, or if a hyperalgesic response is present on the symptomatic side with a normal pain response on the asymptomatic side (Fig. 10-7). For further details on nerve palpation and accessible sites, refer to the publication by Tampin.58

Mechanical hyperalgesia of peripheral nerve trunks has been demonstrated in a subgroup of patients with spinally referred leg pain59 suggesting peripheral nerve sensitization. However, the diagnostic value of nerve trunk palpation is not known. Palpation over a nerve trunk may simultaneously stimulate other tissues such as fascia and muscles that may provoke a pain response.
MUSCULOSKELETAL EXAMINATION
Segmental motion tests of the lumbar spine as well as palpation of spinal structures may aid in determining the cause and localization of the pain (Fig. 10-8). Further musculoskeletal tests, e.g., tests for lumbar motor control or muscle length tests, may be indicated to determine any contributing factors to the patient’s pain condition.

Assessment of Neuropathic Pain
Clinical diagnosis
There is currently no “gold standard” for the diagnosis of neuropathic pain. The diagnosis is based on clinical examination findings and diagnostic tests.45 A grading system with different levels of certainty about the presence of neuropathic pain (no, possible, probable, definite) has been developed by the NeuPSIG19 (Table 10-3). This grading system aims to assist in classifying a presenting pain as being neuropathic pain. The diagnostic approach follows a stepwise process that requires: (1) a neuroanatomically plausible pain distribution and a history suggestive of a relevant neurological lesion or disease, (2) supporting evidence obtained by clinical bedside sensory assessment, i.e. the presence of negative sensory signs with or without positive signs, and (3) an objective diagnostic test confirming the lesion (e.g., neuroimaging (CT, MRI), neurophysiological methods). The pain is defined as “possible” neuropathic pain if the criteria under (1) are met; as “probable” neuropathic pain if criteria (1) and (2) are met, and as “definite” neuropathic pain if all criteria 1-3 are met.19 For pain classified as “probable” neuropathic pain, management should be considered according to the neuropathic pain treatment guidelines.60
| 1) | History of relevant neurological lesion or disease and Pain distribution neuroanatomically plausible |
| Possible neuropathic pain | |
| 2) | Pain associated with sensory signs in the same neuroanatomically plausible distribution |
| Probable neuropathic pain | |
| 3) | Diagnostic tests |
| Definite neuropathic pain |
Based on this grading system, a patient with painful radiculopathy with leg pain would be classified as having probable neuropathic pain if there are negative sensory signs within the pain distribution. The classification of definite neuropathic pain would require a confirmative diagnostic test documenting nerve root compromise. Radicular leg pain without negative sensory signs and without confirmative diagnostic tests would therefore be classified as possible neuropathic pain. This classification may be problematic as patients with radicular pain may have very subtle sensory changes that may not be identified with bedside sensory examination, and/or patients may present mainly with gain of function. This raises the question whether, for these patients, management according to the neuropathic pain treatment guidelines should also be considered, particularly if additional clinical findings confirming a relevant nerve root lesion, such as reflex loss and myotomal weakness, are present.
Neuropathic pain screening tools
Several neuropathic pain screening tools have been developed to assist clinicians and non-specialists in identifying neuropathic pain.61 The questionnaires are based on verbal pain descriptors, with or without items relating to a physical sensory examination (Table 10-4). While there are differences between the tools in the methodology of their developmental and validation studies, certain items seem to overlap and have been considered as “core symptoms” for neuropathic pain, including tingling, numbness, burning, electric shock and touch-evoked pain. The sensitivity of the screening tools ranges from 66% to 85% and specificity from 74% to 90%.61
| PainDETECT | LANSS | S-LANSS | DN4 | NPQ | ID Pain | StEP | |
| Descriptor | |||||||
| Pain constancy | x | x | |||||
| Burning | x | x | x | x | x | x | x |
| Tingling, pins and needles | x | x | x | x | x | x | x |
| Pain evoked by light touch | x | x | x | x | x | ||
| Electric shocks or shooting | x | x | x | ||||
| Pain evoked by heat/cold | x | x | |||||
| Painful cold or freezing pain | x | x | x | ||||
| Numbness | x | x | x | x | x | ||
| Pain evoked by pressure | x | x | |||||
| Itching | x | ||||||
| Autonomic changes | x | x | x | ||||
| Radiation of pain | x | ||||||
| Temporal pain pattern | x | ||||||
| Body chart | x | x | |||||
| Clinical examination | |||||||
| Brush allodynia | x | x | x | ||||
| Decreased response to brush movement | x | ||||||
| Touch hyperaesthesia | x | ||||||
| Pin prick hypoaesthesia | x | x | |||||
| Pin prick hyperaesthesia | x | x | |||||
| Decreased response to blunt pressure | x | ||||||
| Decreased response to cold temperature | x | ||||||
| Cold-evoked pain | x | ||||||
| Temporal summation | x | ||||||
| Pain on straight leg raise testing | x | ||||||
| Self-assessment | |||||||
| Abnormal sensation on rubbing the skin | x | ||||||
| Abnormal sensation with pressure on the skin | x |
The painDETECT,62 the Douleur Neuropathique in 4 questions (DN4)63 and the Standardized Evaluation of Pain (StEP) questionnaire64 have been validated in patients with low back pain. The painDETECT is a self-reported tool consisting of seven weighted sensory descriptor items, plus one item relating to temporal pain characteristics and one item relating to spatial pain characteristics. The questionnaire was developed and validated in a large cohort of 392 German patients and demonstrated a sensitivity of 85% and specificity of 80% in identifying neuropathic pain. However, it has to be mentioned that the English version of painDETECT has not yet been validated in patients with low back/leg pain, and, in fact, the diagnostic accuracy of the English version in patients with neck/arm pain was very limited.65 The DN4 includes interview questions as well as two physical examination items.63 The questionnaire showed high sensitivity (80%) and specificity (92%) in patients with low back with and without leg pain. The original French version of DN4 has been translated into English; however, validation studies of the English DN4 have not yet been reported.
The StEP contains six interview questions and ten physical tests. The questionnaire identified patients with radicular pain with a sensitivity of 92% and specificity of 97%. While these neuropathic pain screening tools have been recommended for use by non-specialists,47 it has to be emphasized that these tools do not replace a careful clinical examination and are not a diagnostic tool.66
Contributing Factors and Screening for Yellow Flags
The above-mentioned evaluation of neuropathic pain, neural integrity and mechanosensitivity are part of a comprehensive clinical reasoning framework incorporating a careful musculoskeletal assessment. Even though it is beyond the scope of this chapter, we would like to highlight the importance of evaluating and addressing contributing factors such as patients’ beliefs, emotional and psychological parameters as well as contextual factors (e.g., yellow, orange, blue or black flags). Importantly, screening for serious pathology (e.g., red flags such as cauda equina syndrome, metastatic spinal cord compression) also forms an integral part of an examination of patients with spinally referred leg pain.
MANAGEMENT OF PATIENTS WITH SPINALLY REFERRED BACK AND LEG PAIN
Multiple guidelines exist for the management of chronic low back pain of somatic origin. Usually, a multimodal approach including exercise, manual therapy, psychological/behavioral interventions and pharmacotherapy is recommended.
The treatment for patients with spinally referred leg pain of neural origin remains challenging. The currently available evidence is based on studies with mostly small sample sizes and high risk of bias. Importantly, the patient populations studied are often heterogeneous with varying eligibility criteria among studies and inconsistent terminology to describe the study population (e.g., radicular pain patients labelled as radiculopathy).67 This contributes to the difficulty in interpreting the already sparse evidence in this field.
The NICE guidelines for low back pain and sciatica68 suggest a period of conservative treatment for patients with lumbar radicular pain with or without radiculopathy before invasive treatments are considered. Indeed, the natural history of acute spinally referred back and leg pain is favorable for most patients; however, up to 49% of patients continue to have symptoms for 6 months or longer.3 Since surgical prognosis worsens with extended preoperative symptom duration,69 understanding the prognostic factors may allow the early identification of patients who may or may not benefit from conservative management. A recent systematic review, however, highlighted that none of the traditionally considered clinical parameters are consistent prognostic factors (e.g., symptom severity and duration, socio-demographics, radiological findings).70 Future studies including either large patient cohorts or smaller but more deeply phenotyped cohorts are needed to determine potential predictors, which may facilitate a stratified treatment approach.
The evidence for efficacy of physiotherapy management strategies for patients with lumbar radicular pain and/or radiculopathy currently remains unclear. There is low quality evidence that in the short-term exercise is superior to advice to stay active, but long-term results are comparable.71 Of note, exercise intervention leads to similar long-term outcomes as surgical intervention. 72 However, surgery produces superior short-term results. Until large and methodologically sound studies are available, physiotherapeutic management has to be based on individual patients’ presentations and the identification of potential contributing factors.
A commonly used physiotherapeutic approach for patients with leg pain of neural origin and features of heightened nerve mechanosensitivity is neurodynamics, which includes interface techniques and neural mobilizations. Foraminal opening techniques are commonly used interface techniques,15 whereas neural mobilization techniques involve passive or active movements, which elongate and shorten the nerve bed. Neural mobilization techniques are broadly differentiated into nerve “sliders” and “tensioners.” “Sliders” are aimed to induce sliding of the peripheral nerves in relation to their surrounding structures with a minimal increase in nerve strain. This is achieved by simultaneous lengthening of the nerve bed at one joint while shortening the nerve bed over another joint. In contrast, “tensioners” aim to increase nerve strain by simultaneously elongating the nerve bed at multiple joints. “Sliders” and “tensioners” may be contraindicated in case of the presence of neuronal damage and high pain severity and irritability. Experimental studies have shown that neural tissue approaches have promising neurophysiological effects including the ability to reduce intraneural swelling and inflammation and increase regeneration capacity.73 Indeed, a recent systematic review concluded that neural tissue management is superior in achieving pain relief and reducing disability levels compared to minimal interventions in patients with spinally referred leg pain and heightened nerve mechanosensitivity. However, neural tissue approaches do not seem more successful than other forms of interventions such as conventional physiotherapy including mobilizations and exercises.74 Of note, there is preliminary evidence that a neurodynamic approach may be particularly effective in patients with heightened nerve mechanosensitivity but significantly less so in patients with radiculopathy, radicular pain or somatically referred pain.75
In patients with neuropathic pain, pharmacological options targeted at neuropathic mechanisms have to be considered. Whereas drugs such as paracetamol and non-steroidal anti-inflammatories target the nociceptive components, they have little effect on neuropathic components. Currently recommended first line treatments for neuropathic pain are tricyclic antidepressants, serotonine-noradrenaline reuptake inhibitors, pregabalin and gabapentin.60 Interestingly, general practitioners seem to identify neuropathic components in patients with radicular pain; however, less than 45% prescribe first line neuropathic pain drugs.76 In contrast, patients with neuropathic pain are often medicated with opioids, even though there is only a weak recommendation for these drugs as a second or third line treatment.60 Unfortunately, systematic reviews suggest no or at best only short-term benefit of commonly used drugs (non-steroidal anti-inflammatories, different neuropathic pain medications) for patients with “sciatica.”77,78 These findings need to be interpreted with caution due to small study samples, inconsistent results and high risk of bias in included trials. Importantly though, most studies include heterogeneous groups of patients (e.g., patients with or without neuropathic pain and with differing sensory profiles), which may have washed out potential effects. To improve pharmacological treatment of patients with neuropathic pain, a mechanism-based approach has been advocated, but extensive research is still required in this area.
More invasive treatments need to be considered if conservative management fails or in the presence of a severe or progressive neurological deficit.
RECOMMENDATIONS
- The terminology used for the description of spinally referred leg pain with a neural component is inconsistently used. Here, we suggest using the following terminology based on pain mechanisms: (1) nociceptive somatic back pain, (2) mixed low back pain (nociceptive and neuropathic), (3) somatic referred pain, (4) neural mechanosensitivity, (5) radicular pain, and (6) radiculopathy (see Fig. 10-1).
- The assessment of patients with spinally referred leg pain includes a comprehensive evaluation of both loss and gain of function in different nerve fiber populations.
- The management of patients with spinally referred leg pain comprises a multidisciplinary effort with physiotherapy and pharmacotherapy being the first line of treatment.
- In patients with neuropathic pain, medications that specifically target neuropathic pain mechanisms should be considered.
SUGGESTED READING
- Baron R, Binder A, Attal N, Casale R, Dickenson AH, Treede RD. Neuropathic low back pain in clinical practice. Eur J Pain. 2016;20(6):861-873.
- Finnerup NB, Attal N, Haroutounian S, et al. Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. Lancet Neurol. 2015;14(2):162-173.
- Finnerup NB, Haroutounian S, Kamerman P, et al. Neuropathic pain: an updated grading system for research and clinical practice. Pain. 2016;157(8): 1599-1606.
- Tampin B, Slater H, Hall T, Lee G, Briffa NK. Quantitative sensory testing somatosensory profiles in patients with cervical radiculopathy are distinct from those in patients with nonspecific neck-arm pain. Pain. 2012;153(12):2403-2414.
- Schmid AB, Nee RJ, Coppieters MW. Reappraising entrapment neuropathies--mechanisms, diagnosis and management. Man Ther. 2013;18(6):449-457.
- Basson A, Olivier B, Ellis R, Coppieters M, Stewart A, Mudzi W. The effectiveness of neural mobilization for neuromusculoskeletal conditions: a systematic review and meta-analysis. J Orthop Sports Phys Ther. 2017;47(9):593-615.
REFERENCES
- Breivik H, Eisenberg E, O'Brien T, OPENminds. The individual and societal burden of chronic pain in Europe: the case for strategic prioritisation and action to improve knowledge and availability of appropriate care. BMC Public Health. 2013;13:1229.
- Konstantinou K, Dunn KM. Sciatica: review of epidemiological studies and prevalence estimates. Spine (Phila Pa 1976). 2008;33(22):2464-2472.
- Hasenbring M, Marienfeld G, Kuhlendahl D, Soyka D. Risk factors of chronicity in lumbar disc patients. A prospective investigation of biologic, psychologic, and social predictors of therapy outcome. Spine (Phila Pa 1976). 1994;19(24):2759-2765.
- Fishbain DA, Cole B, Lewis JE, Gao J. What is the evidence that neuropathic pain is present in chronic low back pain and soft tissue syndromes? An evidence-based structured review. Pain Med. 2014;15(1):4-15.
- Attal N, Perrot S, Fermanian J, Bouhassira D. The neuropathic components of chronic low back pain: a prospective multicenter study using the DN4 Questionnaire. J Pain. 2011;12(10):1080-1087.
- Bouhassira D, Lanteri-Minet M, Attal N, Laurent B, Touboul C. Prevalence of chronic pain with neuropathic characteristics in the general population. Pain. 2008;136(3):380-387.
- Kleinman N, Patel AA, Benson C, Macario A, Kim M, Biondi DM. Economic burden of back and neck pain: effect of a neuropathic component. Popul Health Manag. 2014;17(4):224-232.
- Baron R, Binder A, Attal N, Casale R, Dickenson AH, Treede RD. Neuropathic low back pain in clinical practice. Eur J Pain. 2016;20(6):861-873.
- Attal N, Lanteri-Minet M, Laurent B, Fermanian J, Bouhassira D. The specific disease burden of neuropathic pain: results of a French nationwide survey. Pain. 2011;152(12):2836-2843.
- Bogduk N. On the definitions and physiology of back pain, referred pain, and radicular pain. Pain. 2009;147(1-3):17-19.
- Freynhagen R, Baron R. The evaluation of neuropathic components in low back pain. Curr Pain and Headache Rep. 2009;13(3):185-190.
- Kellgren JH. Referred Pains from Muscle. Br Med J. 1938;1(4023):325-327.
- McCall IW, Park WM, O'Brien JP. Induced pain referral from posterior lumbar elements in normal subjects. Spine (Phila Pa 1976). 1979;4(5):441-446.
- Kellgren JH. On the distribution of pain arising from deep somatic structures with charts of segmental pain areas. Clin Sci. 1939;4:35-46.
- Hall TM, Elvey RL. Nerve trunk pain: physical diagnosis and treatment. Man Ther. 1999;4(2):63-73.
- Marchettini P, Lacerenza M, Mauri E, Marangoni C. Painful peripheral neuropathies. Curr Neuropharmacol. 2006;4(3):175-181.
- Murphy DR, Hurwitz EL, Gerrard JK, Clary R. Pain patterns and descriptions in patients with radicular pain: does the pain necessarily follow a specific dermatome? Chiropr Osteopat. 2009;17:9.
- IASP TFoT. Part III: Pain terms, a current list with definitions and notes on usage. Seattle: IASP Press;1994.
- Finnerup NB, Haroutounian S, Kamerman P, et al. Neuropathic pain: an updated grading system for research and clinical practice. Pain. 2016;157(8):1599-1606.
- Baron R. Neuropathic pain: a clinical perspective. Handb Exp Pharmacol. 2009(194):3-30.
- Behrman M, Linder R, Assadi AH, Stacey BR, Backonja MM. Classification of patients with pain based on neuropathic pain symptoms: comparison of an artificial neural network against an established scoring system. Eur J Pain. 2007;11(4):370-376.
- Bouhassira D, Attal N. Diagnosis and assessment of neuropathic pain: the saga of clinical tools. Pain. 2011;152(3 Suppl):S74-83.
- Jensen MC, Brant-Zawadzki MN, Obuchowski N, Modic MT, Malkasian D, Ross JS. Magnetic resonance imaging of the lumbar spine in people without back pain. N Engl J Med. 1994;331(2):69-73.
- Endean A, Palmer KT, Coggon D. Potential of magnetic resonance imaging findings to refine case definition for mechanical low back pain in epidemiological studies: a systematic review. Spine (Phila Pa 1976). 2011;36(2):160-169.
- Olmarker K, Rydevik B, Holm S, Bagge U. Effects of experimental graded compression on blood flow in spinal nerve roots. A vital microscopic study on the porcine cauda equina. J Orthop Res. 1989;7(6):817-823.
- Lim TK, Shi XQ, Johnson JM, et al. Peripheral nerve injury induces persistent vascular dysfunction and endoneurial hypoxia, contributing to the genesis of neuropathic pain. J Neurosci. 2015;35(8):3346-3359.
- Hida S, Naito M, Kubo M. Intraoperative measurements of nerve root blood flow during discectomy for lumbar disc herniation. Spine (Phila Pa 1976). 2003;28(1):85-90.
- Chew DJ, Leinster VH, Sakthithasan M, Robson LG, Carlstedt T, Shortland PJ. Cell death after dorsal root injury. Neurosci Lett. 2008;433(3): 231-234.
- Schmid AB, Coppieters MW, Ruitenberg MJ, McLachlan EM. Local and remote immune-mediated inflammation after mild peripheral nerve compression in rats. J Neuropathol Exp Neurol. 2013;72(7):662-680.
- Moalem G, Tracey DJ. Immune and inflammatory mechanisms in neuropathic pain. Brain Res Rev. 2006;51(2):240-264.
- Rothman SM, Guarino BB, Winkelstein BA. Spinal microglial proliferation is evident in a rat model of painful disc herniation both in the presence of behavioral hypersensitivity and following minocycline treatment sufficient to attenuate allodynia. J Neurosci Res. 2009;87(12):2709-2717.
- Park HW, Ahn SH, Kim SJ, et al. Changes in spinal cord expression of fractalkine and its receptor in a rat model of disc herniation by autologous nucleus pulposus. Spine (Phila Pa 1976). 2011;36(12):E753-760.
- Kuslich SD, Ulstrom CL, Michael CJ. The tissue origin of low back pain and sciatica: A report of pain responses to tissue stimulation during operations on the lumbar spine using local anaesthesia. Orthop Clin North Am. 1991;22(2):181-187.
- Olmarker K, Rydevik B, Nordborg C. Autologous nucleus pulposus induces neurophysiologic and histologic changes in porcine cauda equina nerve roots. Spine (Phila Pa 1976). 1993;18(11):1425-1432.
- Pedersen LM, Schistad E, Jacobsen LM, Roe C, Gjerstad J. Serum levels of the pro-inflammatory interleukins 6 (IL-6) and -8 (IL-8) in patients with lumbar radicular pain due to disc herniation: a 12-month prospective study. Brain Behav Immun. 2015;46:132-136.
- Schistad EI, Espeland A, Pedersen LM, Sandvik L, Gjerstad J, Roe C. Association between baseline IL-6 and 1-year recovery in lumbar radicular pain. Eur J Pain. 2014;18(10):1394-1401.
- Brisby H, Olmarker K, Larsson K, Nutu M, Rydevik B. Proinflammatory cytokines in cerebrospinal fluid and serum in patients with disc herniation and sciatica. Eur Spine J. 2002;11(1):62-66.
- Albrecht DS, Ahmed SU, Kettner NW, et al. Neuroinflammation of the spinal cord and nerve roots in chronic radicular pain patients. Pain. 2018;159(5):968-977.
- Dilley A, Lynn B, Pang SJ. Pressure and stretch mechanosensitivity of peripheral nerve fibres following local inflammation of the nerve trunk. Pain. 2005;117(3):462-472.
- Bove GM, Light AR. The Nervi Nervorum. Missing link for neuropathic pain? Pain Forum. 1997;6(3):181-190.
- Bove GM, Ransil BJ, Lin HC, Leem JG. Inflammation induces ectopic mechanical sensitivity in axons of nociceptors innervating deep tissues. J Neurophysiol. 2003;90(3):1949-1955.
- Schmid AB, Bland JD, Bhat MA, Bennett DL. The relationship of nerve fibre pathology to sensory function in entrapment neuropathy. Brain. 2014; 137(PT 12):3186-3199.
- Tamburin S, Cacciatori C, Praitano ML, et al. Median nerve small- and large-fiber damage in carpal tunnel syndrome: a quantitative sensory testing study. J Pain. 2011; 12(2):205-212.
- Vrancken AF, Kalmijn S, Brugman F, Rinkel GJ, Notermans NC. The meaning of distal sensory loss and absent ankle reflexes in relation to age: a meta-analysis. J Neurol. 2006;253(5):578-589.
- Council MR. Aids to the investigation of the peripheral nervous system. London: Her Majesty's Stationery Office; Medical Research Council:1943.
- Freynhagen R, Rolke R, Baron R, et al. Pseudoradicular and radicular low-back pain--a disease continuum rather than different entities? Answers from quantitative sensory testing. Pain. 2008;135(1-2):65-74.
- Haanpaa M, Attal N, Backonja M, et al. NeuPSIG guidelines on neuropathic pain assessment. Pain. 2011;152(1):14-27.
- Westermann A, Rönnau AK, Krumova E, et al. Pain-associated mild sensory deficits without hyperalgesia in chronic non-neuropathic pain. Clin J Pain. 2011;27(9):782-789.
- Rolke R, Baron R, Maier C, et al. Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): standardized protocol and reference values. Pain. 2006;123(3):231-243.
- Magerl W, Krumova EK, Baron R, Tölle T, Treede RD, Maier C. Reference data for quantitative sensory testing (QST): refined stratification for age and a novel method for statistical comparison of group data. Pain. 2010;151(3):598-605.
- Pfau DB, Krumova EK, Treede RD, et al. Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): reference data for the trunk and application in patients with chronic postherpetic neuralgia. Pain. 155(5):1002-1015.
- Baron R, Maier C, Attal N, et al. Peripheral neuropathic pain: a mechanism-related organizing principle based on sensory profiles. Pain. 2017;158(2):261-272.
- Nygaard ØP, Kloster R, Solberg T, Mellgren SI. Recovery of function in adjacent nerve roots after surgery for lumbar disc herniation: use of quantitative sensory testing in the exploration of different populations of nerve fibers. J Spinal Disord. 2000;13(5):427-431.
- Tschugg A, Lener S, Hartmann S, et al. Improvement of sensory function after sequestrectomy for lumbar disc herniation: a prospective clinical study using quantitative sensory testing. Eur Spine J. 2016;25:3543-3549.
- Asbury AK, Fields HL. Pain due to peripheral nerve damage: an hypothesis. Neurology. 1984;34(12):1587-1590.
- Gilbert KK, Brismee JM, Collins DL, et al. 2006 Young Investigator Award Winner: lumbosacral nerve root displacement and strain: part 2. A comparison of 2 straight leg raise conditions in unembalmed cadavers. Spine (Phila Pa 1976). 2007;32(14):1521-1525.
- Nee RJ, Jull GA, Vicenzino B, Coppieters MW. The validity of upper-limb neurodynamic tests for detecting peripheral neuropathic pain. J Orthop Sports Phys Ther. 2012;42(5):413-424.
- Tampin B. Integration of peripheral nerves in the examination of the locomotor system. In: Hueter-Becker A, Doelken M, eds. Physical Therapy Examination and Assessment. Vol 1. Stuttgart: Thieme; 2015:76-104.
- Schäfer A, Hall T, Müller G, Briffa K. Outcomes differ between subgroups of patients with low back and leg pain following neural manual therapy: a prospective cohort study. Eur Spine J. 2011;20(3):482-490.
- Finnerup NB, Attal N, Haroutounian S, et al. Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. Lancet Neurol. 2015;14(2):162-173.
- Bennett MI, Attal N, Backonja MM, et al. Using screening tools to identify neuropathic pain. Pain. 2007;127(3):199-203.
- Freynhagen R, Baron R, Gockel U, Tolle TR. painDETECT: a new screening questionnaire to identify neuropathic components in patients with back pain. Curr Med Res Opin. 2006;22(10):1911-1920.
- Bouhassira D, Attal N, Alchaar H, et al. Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN4). Pain. 2005;114(1-2):29-36.
- Scholz J, Mannion RJ, Hord DE, et al. A novel tool for the assessment of pain: validation in low back pain. PLoS Med. 2009;6(4):e1000047.
- Tampin B, Briffa NK, Goucke R, Slater H. Identification of neuropathic pain in patients with neck/upper limb pain: application of a grading system and screening tools. Pain. 2013;154(12):2813-2822.
- Matheison S, Maher CG, Terwee CB, Folly de Campos T, Lin CW. Neuropathic pain screening questionnaires have limited measurement properties. A systematic review. J Clin Epidemiol. 2015; 68(8):957-966.
- Lin CW, Verwoerd AJ, Maher CG, et al. How is radiating leg pain defined in randomized controlled trials of conservative treatments in primary care? A systematic review. Eur J Pain. 2014;18(4):455-464.
- National Guideline Centre (UK). Low back pain and sciatica in over 16s: assessment and management. London; NICE guideline NG59:2016.
- Wilson CA, Roffey DM, Chow D, Alkherayf F, Wai EK. A systematic review of preoperative predictors for postoperative clinical outcomes following lumbar discectomy. Spine J. 2016;16(11):1413-1422.
- Ashworth J, Konstantinou K, Dunn KM. Prognostic factors in non-surgically treated sciatica: a systematic review. BMC Musculoskelet Disord. 2011;12:208.
- Fernandez M, Hartvigsen J, Ferreira ML, et al. Advice to Stay Active or Structured Exercise in the Management of Sciatica: A Systematic Review and Meta-analysis. Spine (Phila Pa 1976). 2015;40(18):1457-1466.
- Fernandez M, Ferreira ML, Refshauge KM, et al. Surgery or physical activity in the management of sciatica: a systematic review and meta-analysis. Eur Spine J. 2016;25(11):3495-3512.
- Schmid AB, Nee RJ, Coppieters MW. Reappraising entrapment neuropathies--mechanisms, diagnosis and management. Man Ther. 2013;18(6):449-457.
- The effectiveness of neural mobilization for neuromusculoskeletal conditions: a systematic review and meta-analysis. J Orthop Sports Phys Ther. 2017;47(9):593-615.
- Schafer A, Hall T, Muller G, Briffa K. Outcomes differ between subgroups of patients with low back and leg pain following neural manual therapy: a prospective cohort study. Eur Spine J. 2011;20(3):482-490.
- Martinez V, Attal N, Vanzo B, et al. Adherence of French GPs to chronic neuropathic pain clinical guidelines: results of a cross-sectional, randomized, "e" case-vignette survey. PLoS One. 2014;9(4):e93855.
- Rasmussen-Barr E, Held U, Grooten WJ, et al. Non-steroidal anti-inflammatory drugs for sciatica. Cochrane Database Syst Rev. 2016;10:CD012382.
- Pinto Rz, Maher CG, Ferreira ML, et al. Drugs for relief of pain in patients with sciatica: systematic review and meta-analysis. BMJ. 2012;34:e497.